
New Work Requirements Put State Medicaid Agencies on the Clock
H.R. 1, often referred to as the “One Big Beautiful Bill Act” (OBBBA), requires Medicaid recipients to meet work requirements to maintain their coverage, which will likely lead to millions of Americans losing their health care. The OBBBA takes effect on January 1, 2027, though states like Nebraska and Montana are implementing them early.[1] These demands have spurred state Medicaid agencies into action, as many are working to develop their guidelines and minimize coverage loss for Medicaid beneficiaries.[2]
Lessons from Medicaid Unwinding: Automation Can Preserve Coverage
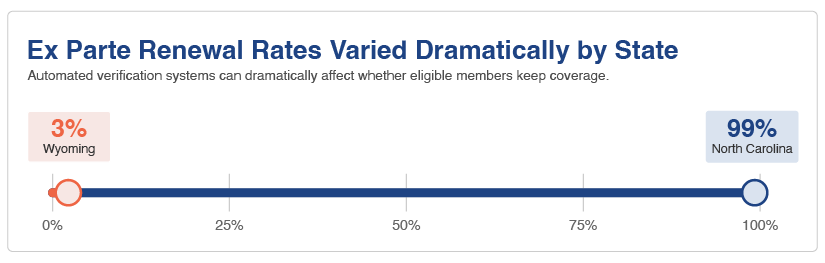
These work requirements pose an unprecedented barrier to Medicaid enrollment, but states have faced mass disenrollment before. When the COVID-19 pandemic wound down, so did Medicaid coverage, as states were no longer required to provide continuous coverage like they were during the public health emergency.[3] To preserve Medicaid coverage, states used ex parte verifications to automatically renew coverage based on reliable data sources like payroll data, state wage or tax databases, or means-tested programs like SNAP. Many states successfully instituted ex parte verification processes, though renewal rates depended heavily on the state, ranging from 99% renewal rates in North Carolina, to just 3% in Wyoming.[4]
States Look to Existing Data to Verify Medical Frailty
Much like with ex parte verification, several state Medicaid agencies are exploring potential data sources for determining medical frailty, which is a key exemption from the new Medicaid work requirements. States like California are prepared to use claims and encounter codes submitted through various service delivery systems for long-term care, Medicaid managed care, and pharmacy benefits. In New York, Gabrielle Armenia, the Director of Division of Eligibility and Marketplace Integration, said the Department of Health is looking to pull coding information from existing data sources that prove medical frailty, such as data that verifies mental health or substance use issues.[5] And in Oklahoma, the Oklahoma Health Care Authority is utilizing automated AI document processing and integrated claims data to screen enrollees to verify eligibility.[6]
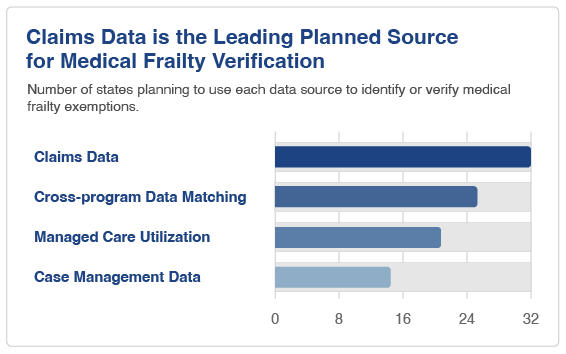
Across the board, states will primarily leverage claims data (32 states) and will match data across programs (25 states). Fewer states will rely on managed care utilization (19 states) or case management data (14 states).[7] Ultimately, states can use these strategies to prevent the burden of verification from falling on Medicaid recipients, thereby preventing their Medicaid coverage from being discontinued.
Self-Attestation Offers a Temporary Pathway
Another approach for confirming medical frailty is self-attestation, where Medicaid members provide a statement verifying their eligibility. CMS issued an interim final rule with comment period (IFC) on June 1, 2026, which clarified that, if the state has no other reliable information, they may accept a statement from applicants or beneficiaries to verify their medical frailty.[8] Self-attestation is allowed through 2027 and once in 2028, but afterwards, Medicaid recipients must provide proof of eligibility when no reliable data is available. Requiring Medicaid recipients to manually submit proof of eligibility will cause many people to lose their coverage in 2028.
Verifying Compliance Before Requesting Documentation
States can utilize existing data sources that demonstrate compliance with work requirements before asking beneficiaries to submit documentation. The types of data sources being considered span across federal, state, and local levels. One type of data that can be used is enrollment records for education, training, and school. The recent rule issued by CMS specifies that applicable individuals must be enrolled at least half-time in a higher education institution, a program for career and technical education, or a high school or high school equivalence program.[9] For instance, California will use various data systems like the California Student Aid Commission and the state Department of Education.[10] This is internal state data that other states could easily emulate when determining compliance.
Another approach would be to use a state’s health information technology infrastructure. During a roundtable in March 2026, New York’s Medicaid Director Amir Bassiri said their statewide health information exchange can be used to exempt populations who may be subject to work requirements. And at a Kentucky forum during May 2026, state staff spoke about potentially using medical records and eligibility records before requesting documentation. CMS is offering states more financial support to improve their eligibility and enrollment systems through private vendors, and less funding to improve states systems, with $200 million in Government Efficiency Grants and over $600 million for private-sector vendors.[11]
States are exploring several types of data sources to verify compliance with the work and community engagement requirements:
- Employment and Wages: California, Louisiana, Massachusetts, and Oklahoma plan to track quarterly state wage data, IRS wage data, and gig economy records.
- Federal Benefits: California and Louisiana will check veteran services history, while Louisiana and Oklahoma will utilize social security data.
- Welfare Systems: California will integrate various welfare systems.
- Community Service: Massachusetts will monitor volunteer and community service registries.
There are plenty of data sources for states to prove compliance, they just need to exercise caution in obtaining consent from consumers when sensitive data is involved.
Importantly, CMS does not appear to treat diagnosis alone as sufficient in all cases. States will need to assess whether the condition significantly impairs the individual’s ability to comply with the 80-hour monthly requirement. However, none of the seven states contacted for this research could answer how they would assess significant impairments. States will likely need to develop practical, defensible processes for assessing functional capacity, using claims and encounter data, diagnosis codes, utilization patterns, provider documentation, screening tools, and other reliable information.
Hardship Exceptions Face Federal Constraints
States may also seek a short-term hardship exception from the work requirements under specific circumstances, like individuals who either receive inpatient or institutional care, reside in a county experiencing an emergency, disaster, or high unemployment, or must travel to receive medical treatment unavailable in their community.[12] As of March 2026, 29 states planned to adopt a hardship exception, with some states planning to adopt some exceptions while not electing others. For instance, New York planned to adopt all exceptions except for patients who must travel for medical treatment, and Oklahoma did not plan to create exemptions for emergencies, disasters, or high unemployment.[13] However, the CMS guidance requires an all-or-nothing approach, where states must either adopt the full set of federally-defined hardship categories, or not allow for any hardship exceptions at all. At a June roundtable, New York’s Medicaid Director Amir Bassiri said they are waiting for additional CMS guidance on operationalizing the exemptions.[14]
Hardship exceptions only provide a narrow pathway for states to exclude Medicaid recipients from work requirements. Exceptions are not only temporary and granted to individuals who are already facing adverse life circumstances, but they are also subject to federal approval. CMS will decide whether a community meets the unemployment threshold based on data published by the Bureau of Labor Statistics (BLS).[15] Exemptions will be requested on a county-by-county basis, which then must go through federal review, requiring substantial cooperation between local, state, and federal agencies.
Outreach Will Be Critical to Reducing Coverage Loss
Many states have begun planning how to best notify Medicaid members about the new work requirements, with many of them relying on staff, community partnerships, and managed care plans to educate beneficiaries. In California and Massachusetts, managed care plan (MCP) representatives already act as primary point of contact for Medicaid members. In New York, Medicaid staff are working with community partners, assistors, health plans, and providers to educate beneficiaries. And Illinois and Louisiana have assembled outreach toolkits for stakeholders to use; Illinois has a multi-phase outreach plan for updating contact information and issuing advance notices for impacted customers, and Louisiana created talking points and graphics for stakeholders to share through various communication channels.
What Policymakers and Advocates Can Do Next
State Medicaid agencies have an uphill battle as they attempt to minimize coverage loss. Within the rigid framework established by the work requirements, legislators and patient advocacy groups could promote measures requiring Medicaid agencies to exhaust every reliable data source possible when proving eligibility and compliance. Further, state Medicaid agencies can hire staff and leverage community partnerships while pursuing outreach methods that target impacted beneficiaries. These approaches could prevent many eligible individuals from losing their coverage due to paperwork, data lags, and justified confusion about the reporting requirements.